Hypermobility and Foot Function
With over 20 years of experience in Podiatry and a clinical focus on Biomechanics, I’ve noticed just how often patients experience foot, leg, knee, hip, and back concerns associated with hypermobility. It is a primary factor in many cases of low arches and pronation-related issues, yet it is often under-discussed in general clinical settings. I have spent several years lecturing in Australia and internationally to postgraduate podiatrists, physiotherapists, chiropractors, and sports doctors about this common condition, its mechanical effects, and clinical management strategies.
HYPER = Too Much, MOBILITY = Range.
Therefore, hypermobility means an increased range in a joint, typically caused by ligamentous laxity. Inherited laxity is due to the ratio and type of collagen in these ligaments; for some, ligaments provide rigid stability, while for others, they are more flexible and elastic.
Your ligaments are effectively the hinges of your body. If you have inherited flexible ligaments, your joints are not held together as tightly as someone with more rigid ligamentous structures.
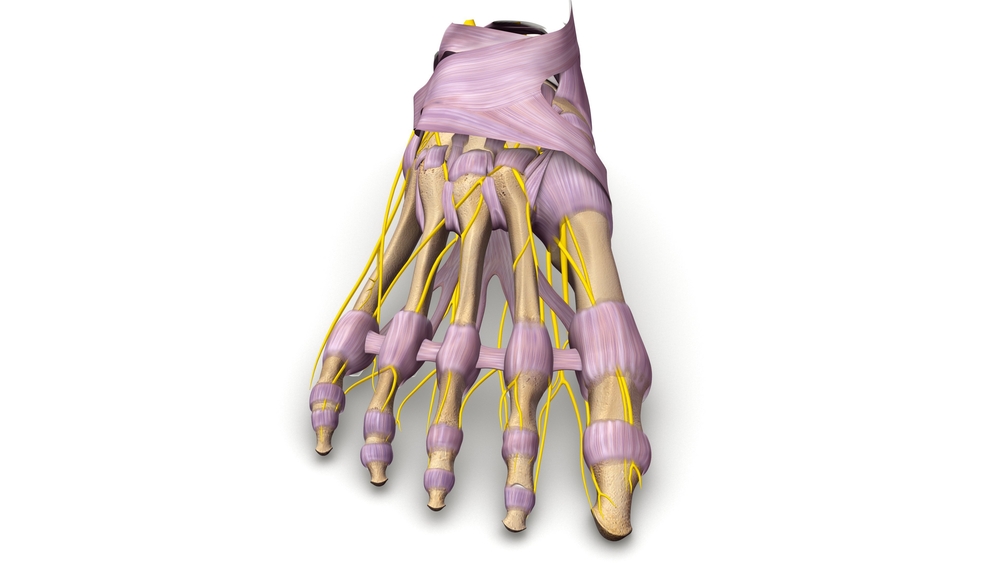
Above is a 3D drawing of the ligaments of the foot
DO NOT CONFUSE HYPERMOBILITY WITH FLEXIBILITY
Flexibility means how much range you have in your muscles and tendons.
This can be altered by stretching (think a ballerina or athlete) which can lengthen muscles and tendons, or by doing weight training or wearing high heels and NEVER stretching which will TIGHTEN them.
Tight muscles will force joints where they don’t want to go, and resist normal motion within joints or overload them. This is why it’s an important part of a management plan to stretch muscles and tendons, especially after exercise, BUT NEVER WHEN COLD. People confuse stretching with warming up. You CAN stretch before exercise, BUT ONLY once you’ve already warmed up (think walking or jogging slowly for several minutes, or lightly spinning on an exercise bike).
Hypermobility means how stretchy your ligaments are
Hypermobility can be GENETIC (family inherited), POST-TRAUMATIC (ligaments stretched in an accident like an ankle sprain, and stay looser or weaker than before) and FUNCTIONAL (think martial artists and dancers stretching to achieve “the splits”).
It can also be HORMONAL for some people, especially females during ovulation when more oestrogen is released, or during pregnancy due to the hormone Relaxin, which helps to loosen the mum’s ligaments to expand her pelvis to let the baby through the birth canal.
Unfortunately, it doesn’t just affect the relevant pelvic ligaments and many women experience joint and muscle pain during late stage pregnancy as their feet aren’t held together as well by these now stretchier ligaments.
HYPERMOBILITY affects a large percentage of people to varying degrees. It is not abnormal or a disease (except in some syndromes like Ehlers Danlos or Marfan’s where the hypermobility is severe and causes great pain and co-ordination problems). It is extremely common in certain racial groups (such as Asians, Indians and Pacific Islanders but occurs in ALL racial groups), but it is a family trait, not a racial one.
If you are “DOUBLE-JOINTED” and your feet hurt, come to Sydney Sports Podiatry and we can provide a clinical assessment to assist you.
SECOND ANKLE SYNDROME

In this picture, you can literally see a foot bending through the midfoot, due to stretchy ligaments (hypermobility).
Midfoot Loading and Hypermobility
This describes the literal folding of the midfoot in patients with genetic, functional or post-traumatic hyper-mobility due to ligament laxity. A more recent term for hypermobility amongst academics is “reduced lower limb soft tissue stiffness”, which essentially means ……HYPERMOBILITY due to ligament laxity!
The feet will literally bend through the arch during contact (for forefoot strikers when running) and propulsion (push-off or toe-off phase from the ground in both runners and walkers). This causes the calf muscles, and especially the lateral gastrocnemius muscles to tighten, causing an increased load to the achilles tendons, calf muscles, and other structures in the feet. My clinical experience of over 25 years has led me to believe calf tightness, secondary to this midfoot loading, can be a significant factor in many foot problems we see.
Come in to Sydney Sports Podiatry if you and /or your family have a history of calf tightness, cramps in the arches or calf muscles, calf tears, forefoot pain, knee pain or discomfort in your feet from standing, walking or running. We can provide a comprehensive assessment to assist you.


